Acetaminophen poisoning
Epidemiology
Leading cause of acute liver failure
Etiology
Pathophysiology
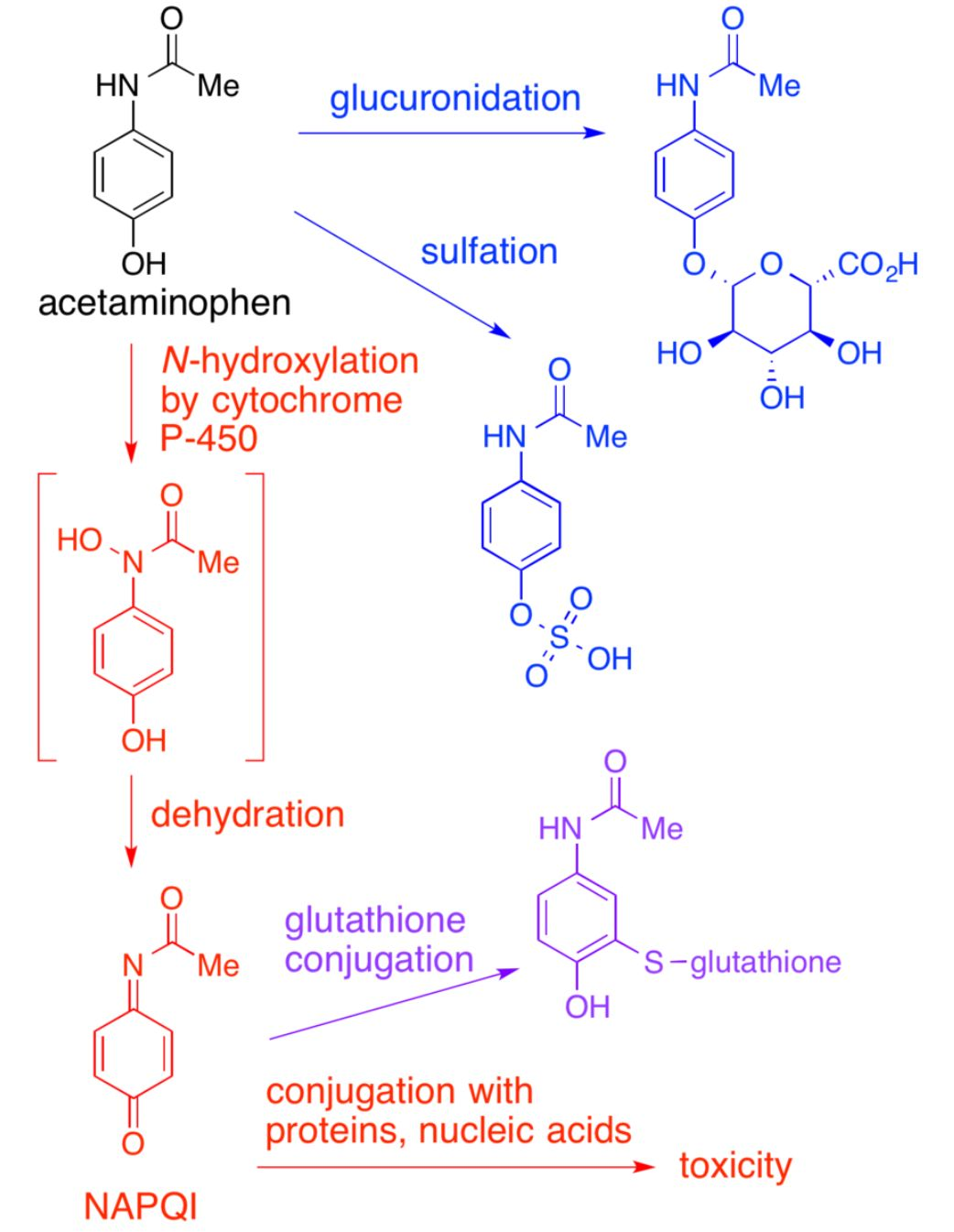
- Exhaustion of hepatic metabolic pathways causes accumulation of a toxic metabolite of acetaminophen, N-acetyl-p-benzoquinoneimine (NAPQI).
- Glutathione initially inactivates NAPQI, but its reserves are eventually depleted, leading to NAPQI accumulation.
- NAPQI → irreversible oxidative hepatocyte injury → liver cell necrosis
- APAP-induced hepatotoxicity
- Defined as peak AST or ALT > 1000 IU/L
- Most commonly caused by APAP overdose
- Occurs rarely at therapeutic doses in patients with:
- Alcohol consumption
- Prolonged fasting
- Chronic liver disease
Clinical features
- Nausea, vomiting
- Pallor
- RUQ pain
- Signs of acute liver failure
Diagnostics
Differential diagnostics
| Feature | Salicylate (ASA) Poisoning | Acetaminophen (APAP) Poisoning | Reye Syndrome |
|---|---|---|---|
| Classic Hx | Overdose (intentional/accidental) | Intentional OD; chronic EtOH use | Child after viral illness + ASA use |
| Pathophysiology | Uncouples ox-phos; Resp center stim; Direct ototoxicity |
Glutathione depletion -> toxic metabolite (NAPQI) -> liver necrosis | Mitochondrial dysfunction -> fatty liver & encephalopathy |
| Presentation | Tinnitus, fever, hyperventilation, AMS | Asymptomatic initially -> RUQ pain -> fulminant liver failure | Profuse vomiting, delirium/coma, NO jaundice |
| Key Lab Finding | Mixed resp. alkalosis + metabolic acidosis | Massive AST/ALT elevation (>1000s) | Hyperammonemia, elevated LFTs, hypoglycemia |
| Antidote / Tx | IV Sodium Bicarbonate, Hemodialysis | N-acetylcysteine (NAC) | Supportive care (manage ICP, hypoglycemia) |
| Buzzword | "Mixed acid-base disorder" | "Rumack-Matthew nomogram" | "Child + virus + aspirin" |
Treatment
- Antidote: PO or IV N-acetylcysteine (NAC) is used to treat and prevent APAP-induced hepatoxicity.
- NAC regenerates glutathione